Fill Out Your Delaware Lq9 Form
Fill Out Your Delaware Lq9 Form
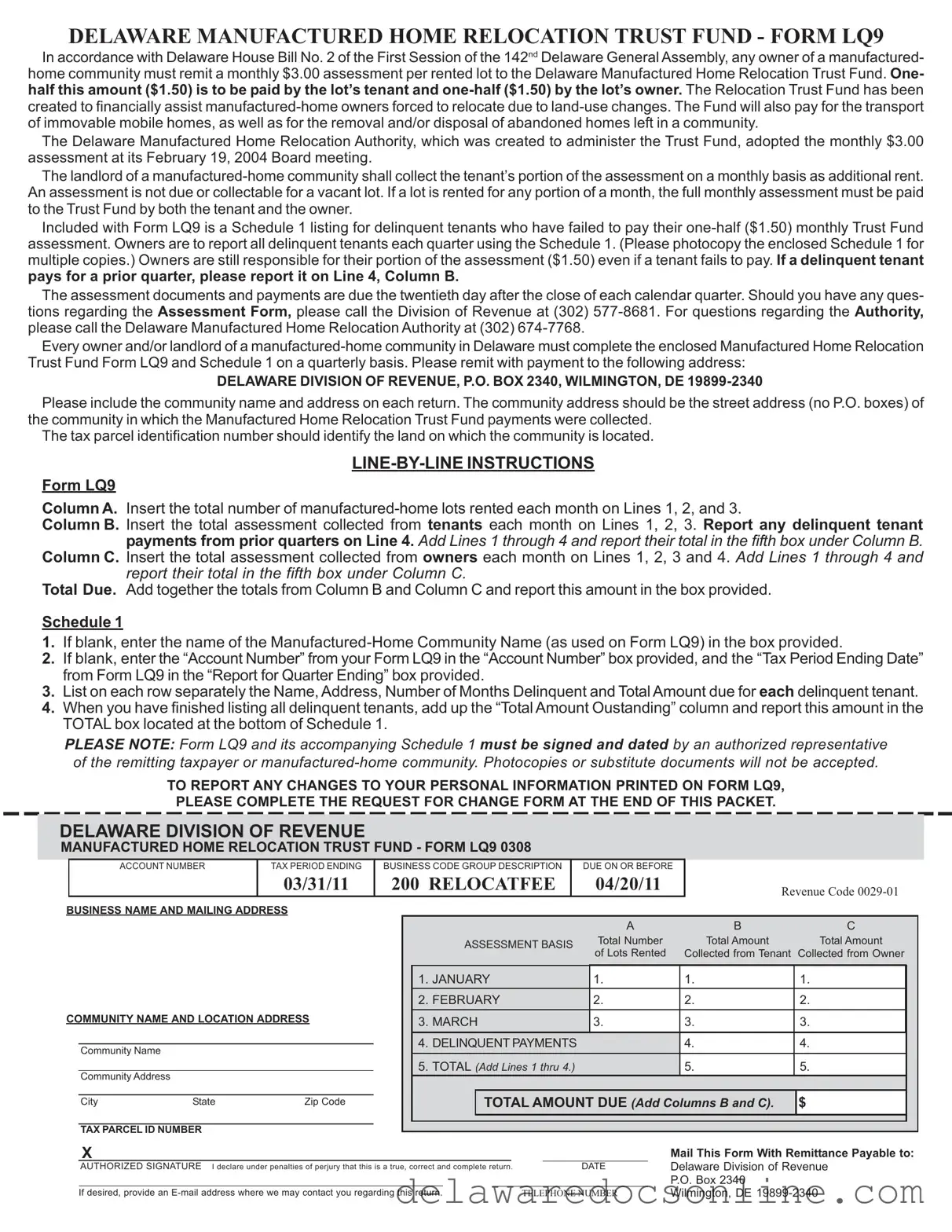
DELAWARE MANUFACTURED HOME RELOCATION TRUST FUND - FORM LQ9
In accordance with Delaware House Bill No. 2 of the First Session of the 142nd Delaware General Assembly, any owner of a manufactured- home community must remit a monthly $3.00 assessment per rented lot to the Delaware Manufactured Home Relocation Trust Fund. One- half this amount ($1.50) is to be paid by the lot’s tenant and
The Delaware Manufactured Home Relocation Authority, which was created to administer the Trust Fund, adopted the monthly $3.00 assessment at its February 19, 2004 Board meeting.
The landlord of a
Included with Form LQ9 is a Schedule 1 listing for delinquent tenants who have failed to pay their
pays for a prior quarter, please report it on Line 4, Column B.
The assessment documents and payments are due the twentieth day after the close of each calendar quarter. Should you have any ques- tions regarding the Assessment Form, please call the Division of Revenue at (302)
Every owner and/or landlord of a
DELAWARE DIVISION OF REVENUE, P.O. BOX 2340, WILMINGTON, DE
Please include the community name and address on each return. The community address should be the street address (no P.O. boxes) of the community in which the Manufactured Home Relocation Trust Fund payments were collected.
The tax parcel identification number should identify the land on which the community is located.
Form LQ9
Column A. Insert the total number of
Column B. Insert the total assessment collected from tenants each month on Lines 1, 2, 3. Report any delinquent tenant payments from prior quarters on Line 4. Add Lines 1 through 4 and report their total in the fifth box under Column B.
Column C. Insert the total assessment collected from owners each month on Lines 1, 2, 3 and 4. Add Lines 1 through 4 and report their total in the fifth box under Column C.
Total Due. Add together the totals from Column B and Column C and report this amount in the box provided.
Schedule 1
1.If blank, enter the name of the
2.If blank, enter the “Account Number” from your Form LQ9 in the “Account Number” box provided, and the “Tax Period Ending Date” from Form LQ9 in the “Report for Quarter Ending” box provided.
3.List on each row separately the Name, Address, Number of Months Delinquent and Total Amount due for each delinquent tenant.
4.When you have finished listing all delinquent tenants, add up the “Total Amount Oustanding” column and report this amount in the TOTAL box located at the bottom of Schedule 1.
PLEASE NOTE: Form LQ9 and its accompanying Schedule 1 must be signed and dated by an authorized representative of the remitting taxpayer or
TO REPORT ANY CHANGES TO YOUR PERSONAL INFORMATION PRINTED ON FORM LQ9,
PLEASE COMPLETE THE REQUEST FOR CHANGE FORM AT THE END OF THIS PACKET.
DELAWARE DIVISION OF REVENUE
MANUFACTURED HOME RELOCATION TRUST FUND - FORM LQ9 0308
|
|
ACCOUNT NUMBER |
TAX PERIOD ENDING |
BUSINESS CODE GROUP DESCRIPTION |
|
DUE ON OR BEFORE |
|
|
|
|
||||||||||||||||
|
|
|
|
03/31/11 |
200 RELOCATFEE |
|
04/20/11 |
|
|
REVENUE CODE |
|
|||||||||||||||
BUSINESS NAME AND MAILING ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
B |
C |
|
|||
|
|
|
|
|
|
|
|
|
ASSESSMENT BASIS |
|
Total Number |
|
|
Total Amount |
Total Amount |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
of Lots Rented |
|
|
Collected from Tenant |
Collected from Owner |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
JANUARY |
|
|
|
|
|
1. |
|
|
|
1. |
1. |
|
|
|||||
|
|
|
|
|
|
|
2. |
FEBRUARY |
|
|
|
|
|
2. |
|
|
|
2. |
2. |
|
|
|||||
COMMUNITY NAME AND LOCATION ADDRESS |
|
|
3. |
MARCH |
|
|
|
|
|
3. |
|
|
|
3. |
3. |
|
|
|||||||||
|
|
|
|
|
|
|
4. |
DELINQUENT PAYMENTS |
|
|
|
|
|
4. |
4. |
|
|
|||||||||
|
|
Community Name |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
5. |
TOTAL (Add Lines 1 thru 4.) |
|
|
|
|
|
5. |
5. |
|
|
|||||||||
|
|
Community Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
TOTAL AMOUNT DUE (Add Columns B and C). |
$ |
|
|
|||||||||||||
|
|
City |
State |
Zip Code |
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TAX PARCEL ID NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mail This Form With Remittance Payable to: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
AUTHORIZED SIGNATURE I declare under penalties of perjury that this is a true, correct and complete return. |
|
|
|
|
DATE |
Delaware Division of Revenue |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P.O. Box 2340 |
|
|
|
||
|
|
If desired, provide an |
TELEPHONE NUMBER |
Wilmington, DE |
|
|||||||||||||||||||||
DELAWARE DIVISION OF REVENUE
MANUFACTURED HOME RELOCATION TRUST FUND - FORM LQ9 0308
|
|
|
|
|
|
|
|
ACCOUNT NUMBER |
|
|
TAX PERIOD ENDING |
|
|
BUSINESS CODE GROUP DESCRIPTION |
DUE ON OR BEFORE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
06/30/11 |
|
|
|
|
|
200 RELOCATFEE |
07/20/11 |
|
|
|
|
|
|
|
|
|
|
|
|
REVENUE CODE |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
BUSINESS NAME AND MAILING ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
B |
|
|
|
|
|
C |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ASSESSMENT BASIS |
|
|
|
Total Number |
|
|
Total Amount Collected |
|
|
|
Total Amount |
|
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
of Lots Rented |
|
|
|
|
from Tenant |
Collected from Owner |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
APRIL |
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
MAY |
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
COMMUNITY NAME AND LOCATION ADDRESS |
|
|
|
|
|
3. |
JUNE |
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
DELINQUENT PAYMENTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
Community Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
TOTAL (Add Lines 1 thru 4.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
Community Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL AMOUNT DUE (Add Columns B and C). |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
City |
|
State |
|
|
|
|
|
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TAX PARCEL ID NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mail This Form With Remittance Payable to: |
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
AUTHORIZED SIGNATURE I declare under penalties of perjury that this is a true, correct and complete return. |
|
|
|
|
|
|
|
|
|
DATE |
Delaware Division of Revenue |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P.O. Box 2340 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
If desired, provide an |
TELEPHONE NUMBER |
Wilmington, DE |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DELAWARE DIVISION OF REVENUE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
MANUFACTURED HOME RELOCATION TRUST FUND - FORM LQ9 0308 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
ACCOUNT NUMBER |
|
|
TAX PERIOD ENDING |
|
|
BUSINESS CODE GROUP DESCRIPTION |
DUE ON OR BEFORE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
09/30/11 |
|
|
|
|
|
200 RELOCATFEE |
10/20/11 |
|
|
|
|
|
|
|
|
|
|
|
|
REVENUE CODE |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
BUSINESS NAME AND MAILING ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
B |
|
|
|
|
|
C |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ASSESSMENT BASIS |
|
|
|
Total Number |
|
|
Total Amount Collected |
|
|
|
Total Amount |
|
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
of Lots Rented |
|
|
|
|
from Tenant |
Collected from Owner |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
JULY |
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
AUGUST |
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
COMMUNITY NAME AND LOCATION ADDRESS |
|
|
|
|
|
3. |
SEPTEMBER |
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
DELINQUENT PAYMENTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
Community Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
TOTAL (Add Lines 1 thru 4.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
Community Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL AMOUNT DUE (Add Columns B and C). |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
City |
|
State |
|
|
|
|
|
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TAX PARCEL ID NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mail This Form With Remittance Payable to: |
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
AUTHORIZED SIGNATURE I declare under penalties of perjury that this is a true, correct and complete return. |
|
|
|
|
|
|
|
|
|
DATE |
Delaware Division of Revenue |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P.O. Box 2340 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
If desired, provide an |
TELEPHONE NUMBER |
Wilmington, DE |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DELAWARE DIVISION OF REVENUE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
MANUFACTURED HOME RELOCATION TRUST FUND - FORM LQ9 0308 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
ACCOUNT NUMBER |
|
|
TAX PERIOD ENDING |
|
|
BUSINESS CODE GROUP DESCRIPTION |
DUE ON OR BEFORE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12/31/11 |
|
|
|
|
|
200 RELOCATFEE |
01/20/12 |
|
|
|
|
|
|
|
|
|
|
|
|
REVENUE CODE |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
BUSINESS NAME AND MAILING ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
B |
|
|
|
|
|
C |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ASSESSMENT BASIS |
|
|
|
Total Number |
|
|
Total Amount Collected |
|
|
|
Total Amount |
|
|
|||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
of Lots Rented |
|
|
|
|
from Tenant |
Collected from Owner |
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
OCTOBER |
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
NOVEMBER |
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
COMMUNITY NAME AND LOCATION ADDRESS |
|
|
|
|
|
3. |
DECEMBER |
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
DELINQUENT PAYMENTS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
Community Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
TOTAL (Add Lines 1 thru 4.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
Community Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TOTAL AMOUNT DUE (Add Columns B and C). |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
City |
|
State |
|
|
|
|
|
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TAX PARCEL ID NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mail This Form With Remittance Payable to: |
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
AUTHORIZED SIGNATURE I declare under penalties of perjury that this is a true, correct and complete return. |
|
|
|
|
|
|
|
|
|
DATE |
Delaware Division of Revenue |
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P.O. Box 2340 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
If desired, provide an |
TELEPHONE NUMBER |
Wilmington, DE |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

DELAWARE MANUFACTURED HOME RELOCATION TRUST FUND
Schedule 1 - Delinquent Tenant Report
ACCOUNT NUMBER |
REPORT FOR QUARTER ENDING: |
||
COMMUNITY OWNER |
|||
|
|
||
|
|
|
NAME OF DELINQUENT TENANT |
STREET ADDRESS |
CITY |
STATE |
ZIP CODE |
|
|
|
|
|
|
|
|
|
|
BUSINESS CODE GROUP DESCRIPTION
200 RELOCATFEE
NUMBER OF MONTHS |
TOTAL AMOUNT |
DELINQUENT |
OUTSTANDING |
TOTAL
$
Mail This Form With Remittance Payable To:
Delaware Division of Revenue
P.O. Box 2340, Wilmington, DE
AUTHORIZED SIGNATURE I declare under penalties of perjury, that this |
DATE |
TELEPHONE NUMBER |
|
is a true, correct and complete return. |
|
|
|
Delaware Manufactured Home Relocation Trust Fund - Form LQ9
Request for Change Form
Use this form to make corrections or changes to your name, address, account number or taxable
 Please Note: This Request for Change form only makes changes to your account in our Business Master File. If you need to make similar changes to any other accounts (Corporate, Sub S Corporate, License and/or Withholding accounts), please complete the Corporate Request for Change form, the Sub S Corporate Request for Change form, the License Request for Change form or the Withholding Request for Change form respectively for each type of tax. These forms can be found on our website at: www.revenue.delaware.gov.
Please Note: This Request for Change form only makes changes to your account in our Business Master File. If you need to make similar changes to any other accounts (Corporate, Sub S Corporate, License and/or Withholding accounts), please complete the Corporate Request for Change form, the Sub S Corporate Request for Change form, the License Request for Change form or the Withholding Request for Change form respectively for each type of tax. These forms can be found on our website at: www.revenue.delaware.gov.
Step 1: Please enter your information as it appears on the Division of Revenue’s current records
Box A. Account Number – Please enter the Federal Tax Identification Number that the Delaware Division of Revenue currently has on file for you.
Box B. Business Name and Address – Please enter the business name and location address that the Delaware Division of Revenue currently lists as your business name and location address.
Step 2:
Field 1. Correct Business Activity – If you have changes to your current business activity, please enter your new or corrected business activity in Field 1.
Field 2. Account Number Change – If you wish to change the information in Box A, please enter your correct account number in Field 2. Otherwise, leave Field 2 blank.
Field 3. Effective Date – Please enter the date you would like this Request for Change form to go into effect. Field 4. Reason for Change – Please enter the reason for submitting this Request for Change form (i.e. out
of business, incorporated, moved).
Field 5. Sole Propietors Only – Please enter your current Social Security Number if you are a sole proprietor. If you are not a sole proprietor, please leave Field 5 blank.
Field 6. Correct Community Address – If you wish to change the information in Box B, please enter your correct location address in Field 6. Otherwise, leave Field 6 blank.
Field 7. Correct Mailing Address – Please enter your correct mailing address.
Step 3: Sign and date the form. Mail to the address listed on the form or fax to
If you have any questions, please call the Delaware Division of Revenue Business Master File Section at
|
DELAWARE DIVISION OF REVENUE |
REQUEST FOR CHANGE |
|
|
LREQ |
|||||||
|
PO BOX 8750 |
|
|
New Booklets Will Be Issued |
|
|
||||||
|
WILMINGTON, DE |
for Account No. & Bus. Code Group Changes Only |
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
REVENUE CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. CORRECT BUSINESS ACTIVITY |
|
2. ACCOUNT NUMBER CHANGE |
3. EFFECTIVE DATE |
4. REASON FOR CHANGE |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
BUSINESS CODE GROUP DESCRIPTION |
|
A. ACCOUNT NUMBER |
6. CORRECT BUSINESS LOCATION ADDRESS |
|
||||||||
|
200 RELOCATFEE |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
SOLE PROPRIETORS: ENTER |
|
|
|
|
|
|||||
B. BUSINESS NAME |
|
SOCIAL SECURITY NUMBER |
|
|
|
|
|
|||||
|
|
|
|
|
ADDRESS |
|
|
|
|
|||
|
AND MAILING ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITY |
|
STATE |
ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. CORRECT MAILING ADDRESS IF DIFFERENT FROM ABOVE |
|
|||
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AUTHORIZED SIGNATURE |
|
|
DATE |
|
|
|
|
|
|||
|
|
|
CITY |
|
STATE |
ZIP CODE |
|
|||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE NUMBER |
Completing the Delaware LQ9 form is essential for owners of manufactured-home communities. This process involves gathering specific information about rented lots and assessments collected from tenants and owners. Following the steps outlined below will help ensure that the form is filled out accurately and submitted on time.
Following these steps will help you complete the LQ9 form correctly and meet the requirements for submission. Be mindful of the deadlines to avoid any penalties. If you have questions, don't hesitate to reach out to the Division of Revenue for assistance.
The Delaware LQ9 form is an essential document for owners of manufactured-home communities, ensuring compliance with state regulations regarding the Manufactured Home Relocation Trust Fund. Alongside this form, several other documents are commonly used to facilitate the assessment and management of the Trust Fund. Here’s a brief overview of these related forms and documents.
Each of these documents plays a vital role in the administration of the Manufactured Home Relocation Trust Fund in Delaware. They help ensure that owners remain compliant with state regulations while also providing necessary support to tenants facing relocation. Proper handling of these forms can prevent potential issues and facilitate smoother operations within manufactured-home communities.
1. Monthly Assessment Requirement: Every owner of a manufactured-home community in Delaware must collect a monthly assessment of $3.00 per rented lot. This amount is split equally between the tenant and the owner, with each responsible for $1.50.
2. Reporting Delinquent Tenants: Owners must report any tenants who fail to pay their portion of the assessment using Schedule 1. This report is due quarterly and should include details such as the tenant's name, address, and the total amount owed.
3. Payment Deadlines: All assessment documents and payments must be submitted by the twentieth day after the close of each calendar quarter. Timely submission is crucial to avoid penalties.
4. Accurate Completion of Form LQ9: Owners must ensure that Form LQ9 is filled out correctly, including the total number of lots rented and the total amounts collected from both tenants and owners. Inaccuracies can lead to complications in reporting and compliance.
Delaware Corporate Tax Return - Corporations reporting a federal taxable income under $10 million use this simplified tax return.
This document is crucial for individuals engaging in ATV transactions, providing a clear framework through the detailed California ATV Bill of Sale form requirements that ensure both parties are protected during the sale process.
Delaware Pardon Application - Visit the Board of Pardons website for additional information and resources.
| Fact Name | Details |
|---|---|
| Monthly Assessment Amount | The monthly assessment for the Delaware Manufactured Home Relocation Trust Fund is $3.00 per rented lot. |
| Payment Split | This amount is split equally, with $1.50 paid by the tenant and $1.50 by the lot owner. |
| Purpose of the Fund | The Trust Fund assists manufactured-home owners who need to relocate due to land-use changes. |
| Delinquent Tenant Reporting | Owners must report delinquent tenants quarterly using Schedule 1, which is included with Form LQ9. |
| Assessment Collection | Landlords collect the tenant’s portion as additional rent each month. |
| Vacant Lots | No assessment is due for vacant lots. If a lot is rented for any part of a month, the full assessment is owed. |
| Governing Law | This form is governed by Delaware House Bill No. 2 from the 142nd Delaware General Assembly. |