Fill Out Your Delaware Uc 400 Form
Fill Out Your Delaware Uc 400 Form
Delaware Department of Labor |
|
Division of Unemployment Insurance |
Document |
PO Box 9953 |
|
Wilmington, DE |
|
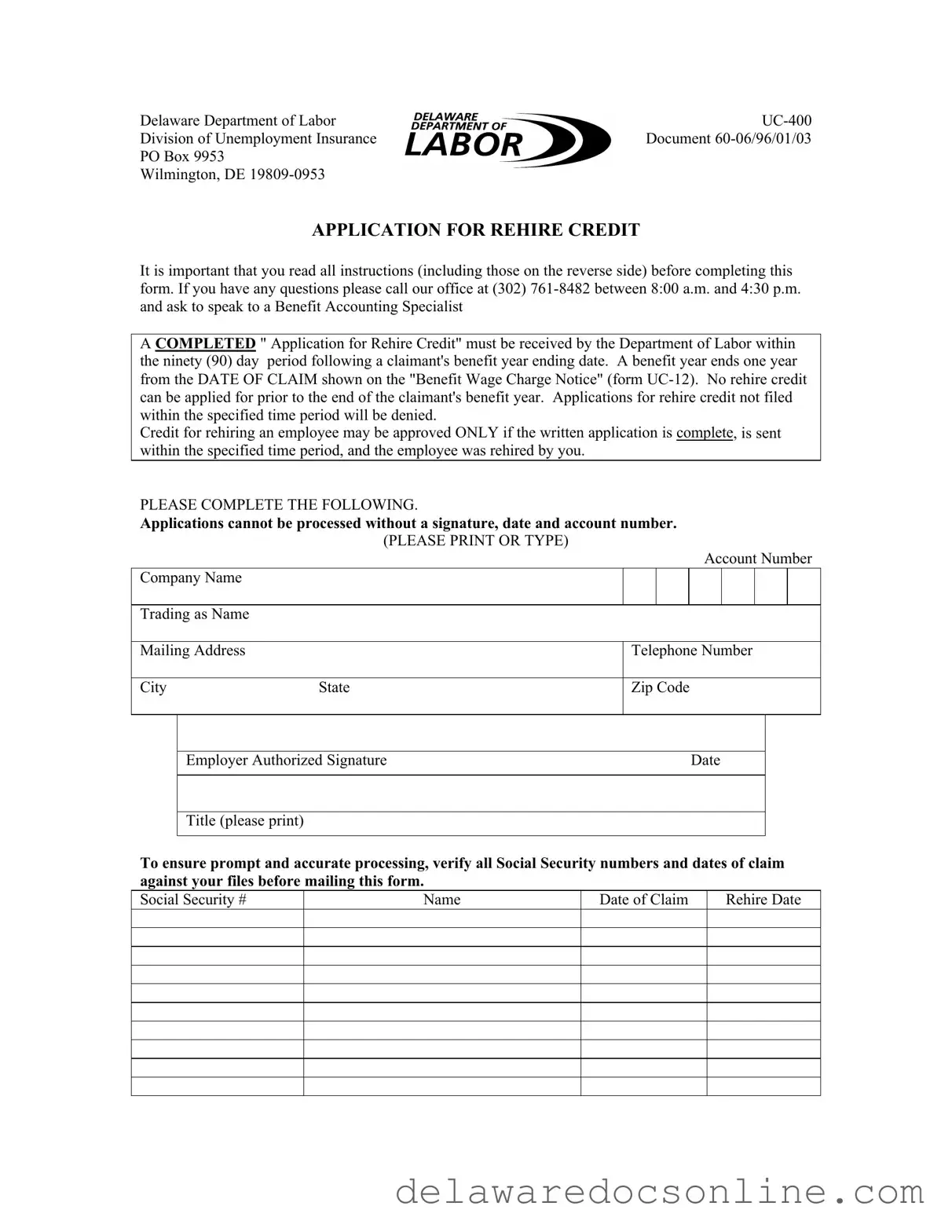
APPLICATION FOR REHIRE CREDIT
It is important that you read all instructions (including those on the reverse side) before completing this form. If you have any questions please call our office at (302)
A COMPLETED " Application for Rehire Credit" must be received by the Department of Labor within the ninety (90) day period following a claimant's benefit year ending date. A benefit year ends one year from the DATE OF CLAIM shown on the "Benefit Wage Charge Notice" (form
Credit for rehiring an employee may be approved ONLY if the written application is complete, is sent within the specified time period, and the employee was rehired by you.
PLEASE COMPLETE THE FOLLOWING.
Applications cannot be processed without a signature, date and account number.
|
|
(PLEASE PRINT OR TYPE) |
|
|
|
|
|
|
|
|
|
|
|
|
Account Number |
||||
Company Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trading as Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Mailing Address |
|
Telephone Number |
|||||||
|
|
|
|
|
|||||
City |
State |
Zip Code |
|||||||
|
|
|
|
|
|
||||
|
|
|
|
|
|
||||
|
Employer Authorized Signature |
|
|
Date |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Title (please print) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To ensure prompt and accurate processing, verify all Social Security numbers and dates of claim against your files before mailing this form.
Social Security # |
Name |
Date of Claim |
Rehire Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Completing the Delaware UC-400 form is a straightforward process, but it requires attention to detail. Make sure to gather all necessary information before you begin. This form must be submitted within 90 days after the end of the claimant's benefit year. Follow these steps to ensure your application is filled out correctly.
After completing the form, double-check all entries for accuracy. Ensure that the form is signed and dated. Submit it to the Delaware Department of Labor within the required timeframe for processing.
The Delaware UC-400 form is an important document for employers seeking rehire credits for employees who have previously claimed unemployment benefits. Alongside this form, several other documents are often required or beneficial for a complete application process. Below is a list of related forms and documents that may be used in conjunction with the UC-400.
By understanding these related forms and documents, employers can navigate the rehire credit application process more effectively. Ensuring all necessary paperwork is completed accurately and submitted on time will help in obtaining the desired credit for rehiring employees.
Here are some key takeaways about filling out and using the Delaware UC-400 form:
Delaware Quarterly Taxes - Filing this form is mandatory for both resident and non-resident fiduciaries when applicable.
An Employment Verification Form is a document used by employers to confirm the employment status of current or former employees. This form typically includes information such as the employee's position, dates of employment, and sometimes, salary details. It serves as a critical tool for various purposes, including background checks for new employment, loan applications, and housing requests, and you can find a useful template at TopTemplates.info.
Does Delaware Tax Social Security - Delaware taxpayers must fill out the 1089 accurately to avoid delays.
| Fact Name | Description |
|---|---|
| Form Purpose | The UC-400 form is used to apply for rehire credit for employees who have previously received unemployment benefits. |
| Governing Law | This form is governed by Delaware's Unemployment Insurance laws. |
| Submission Deadline | Applications must be submitted within 90 days after the claimant's benefit year ends. |
| Eligibility | Rehire credit is only granted if the employee was rehired and the application is complete. |
| Contact Information | For questions, contact the Delaware Department of Labor at (302) 761-8482. |
| Signature Requirement | A valid signature, date, and account number are mandatory for processing the application. |
| Verification | Ensure all Social Security numbers and claim dates are accurate before submitting the form. |